

多参数磁共振(multiparametric magnetic resonance imaging, mpMRI)已被广泛用于评估前列腺肿瘤分期以及PLNM预测[4-5],肿瘤原发灶的位置信息和形态特征可以提高PLNM预测性能[6-
本文开发了一种注意力引导的多任务网络,通过整合来自前列腺肿瘤分割网络中小尺度和大尺度特征,提取肿瘤的局部和全局空间信息,从而提升前列腺癌PLNM预测精度.该网络包括两部分:一个基于多分支各向异性大核注意力模块的前列腺肿瘤分割网络,用来捕捉不同感受野下的原发肿瘤内部异质性的局部和全局特征;以及一个基于多尺度特征交互融合注意力模块的PLNM预测网络.该预测网络有选择地利用多尺度特征来细化单尺度特征,通过对相邻尺度特征中每个像素进行加权,确保充分的多尺度特征融合,并筛选出高鉴别性的分类特征.最后,使用加权的多任务损失函数来平衡分割和分类任务的性能.在320例前列腺癌数据集上的实验结果显示,该方法在PLNM预测方面具有较好的应用前景.
1 预测方法
1.1 概述
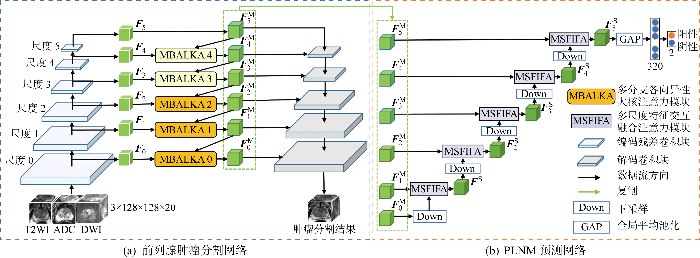
图1所示为所提三维注意力引导多任务学习的 PLNM 预测.Fn, n∈{0, 1, 2, 3, 4, 5}代表分割网络产生的粗略多尺度特征;FMn, n∈{0, 1, 2, 3, 4, 5}代表由多分支各向异性大核注意力(multi-branch anisotropic large kernel attention, MBALKA)模块获得的共享多尺度特征; FSn, n∈{1, 2, 3, 4, 5}代表由多尺度特征交互融合注意力(multi-scale feature interaction fusion attention, MSFIFA)模块得到的融合多尺度特征.三维网络以前列腺区域mpMRI影像(T2WI、ADC、DWI)为输入,以前列腺肿瘤分割结果和PLNM预测结果为输出.PLNM预测任务可视为一项分类任务,即将患者分为有或无PLNM.3D DynUnet[15]被用来作为多任务网络骨干,它可以根据数据集的特点配置各向异性的卷积核和合适的下采样步幅,从而获取不同分辨率的粗略多尺度特征.
图1
1.2 基于MBALKA模块的前列腺肿瘤分割网络
在多任务网络中,PLNM预测与前列腺肿瘤分割任务相结合,以探索肿瘤内部异质性.肿瘤分割网络如图1(a)所示,左半部分是编码器,为分割和分类任务提取共同特征;右半部分是解码器,通过跳跃连接接收共同特征并进行肿瘤分割.MBALKA模块的目标是充分挖掘不同尺度特征中肿瘤的局部和全局三维空间信息,其设计灵感来源于大核注意力[16],它吸收了卷积和自注意力[17]的局部结构信息和长程依赖性等优点,虽然大核注意力取得了不错的效果,但忽略了不同感受野和不同尺度特征聚合的作用.与大核注意力不同,本文不仅将大卷积核推广到多分支结构,还在不同分支中设置不同尺寸(图1(a)中分支颜色不同表示结构不同)的各向异性卷积核,并引入注意力机制,从而同时提取不同感受野中肿瘤的局部和全局特征.此外,根据不同尺度设置了不同的分支,以进一步丰富感受野.所设计的MBALKA模块嵌入了自上而下的特征融合策略,以有效地整合高层次的语义信息和低层次的细节信息,并通过不同尺寸各向异性的大卷积核形成具有不同感受野的多分支注意特征池,具体结构如图2所示.图中:fn表示第n个MBALKA模块;“upsample”代表上采样操作;
图2

图2(a)展示了MBALKA0结构,其中包括多分支特征池的所有细节.MBALKA1和MBALKA2与MBALKA0结构相同,由于深层特征图尺寸较小,过大的卷积核会获得较多的无关信息,所以为了适应不同尺度特征图的尺寸,MBALKA3只保留3个分支Branch1~Branch3,MBALKA4只保留两个分支Branch1和Branch2.图2(b)为MBALKA0中Branch2结构,通过组合3×3×1的深度卷积(depth-wise convolution,DWConv)、5×5×3的深度扩张卷积(depth-wise dilation convolution,DWDConv)和1×1×1的通道卷积(point-wise convolution,PWConv),形成近似一个9×9×5的大卷积核,从而获取更大的感受野.本文MBALKA模块能够提取相邻尺度中肿瘤的局部和全局的特征,其在不同尺度特征下的特征提取过程如下:
式中:
1.3 基于MSFIFA模块的PLNM预测网络
式中:“downsample”代表下采样操作;f(·)代表 MSFIFA 模块;PGA代表全局平均池化(GAP)操作;Pc代表第c类样本的输出概率.
虽然MBALKA模块获得了共享多尺度特征,但小尺度特征中的高层次语义信息和大尺度特征中丰富的细节信息在相互转移时不可避免地会受到来自非目标区域的噪声干扰.因此,设计MSFIFA模块,一方面进一步突出原发肿瘤的特征,另一方面通过对每个像素加权来确保充分的多尺度特征融合并筛选出高鉴别性的分类特征.
图3显示了MSFIFA模块的详细结构,两个输入特征图
图3

1.4 多任务总损失
总损失函数由两部分组成,包括前列腺肿瘤分割的分割损失和PLNM预测的分类损失.对于前列腺肿瘤分割,使用一种混合损失函数,由Dice Loss(LDice)和Focal Loss (LFocal)函数组成.对于PLNM预测任务,选择交叉熵损失函数(LCE)作为分类损失.目前,常见的多任务学习方法是优化所有任务的线性加权损失并求解最小值.然而,这种方法权重参数设置繁琐.为了减轻分割任务和分类任务之间由于权重设置不当导致的分类精度降低的影响,采用基于不确定性的方法[18]来自适应权衡前列腺肿瘤分割和PLNM预测任务的损失.最后,多任务总损失函数定义如下:
式中,σSeg和σClass为不确定权重,通过网络进行学习.实际应用中,σSeg和σClass先被初始化为1,然后在训练阶段通过迭代进行自适应更新.
2 数据和实施细节
2.1 数据集
本文数据集由苏州大学附属第二人民医院通过飞利浦3.0 T mpMRI收集,面内分辨率为0.31~0.49 mm,切片间距为3~3.5 mm;包含320个mpMRI图像样本,收集时间为2015年1月~2022年3月,并进行随访至2023年3月.同时满足以下条件的患者被接受:①临床或病理诊断为前列腺癌;②诊断时均保留3种模态(T2WI、ADC、DWI)的 mpMRI 影像;③患者的穿刺病理和手术病理均无缺失.该研究通过了苏州大学附属第二医院伦理委员会的审批(批文编号:JD-HG-2021-31)并已获得患者的书面知情同意,他们的匿名信息将在本文中发表.分割的真实标签由3位经验丰富的放射科医生基于手术病理结果使用ITK-SNAP软件进行注释.分类标签来自医生提供的手术病理结果的统计数据,其中229个样本为PLNM阴性,剩余91个样本为 PLNM 阳性.
2.2 数据预处理
使用开源的Elastix软件[19]进行3种模态(T2WI、ADC、DWI)的图像配准.为了减少前列腺以外背景区域的干扰,通过图4所示流程裁剪出前列腺感兴趣区域.首先,使用经过前列腺数据预训练的前列腺自动分割网络nn-Unet[20]获得前列腺分割标签;然后,根据前列腺分割标签生成前列腺边界框并外扩1 cm;最后,将每个样本的图像裁剪出前列腺感兴趣区域.利用双线性插值将所有样本的mpMRI影像重新采样到样本切片间距的中等分辨率(0.464, 0.464, 3) mm,为应对三维数据对计算机内存消耗的限制,将图像调整大小到128像素×128像素×20像素,为了提高模型的泛化能力,训练图像被归一化为(0, 1).
图4

2.3 训练过程
提出的模型在PyTorch平台上实现,使用NVIDIA GeForce 3090Ti GPU(24 GB),采用五折交叉验证策略进行训练,每个类标签的比例相同.为体现客观性,所有实验均采用上述策略;所有模型均使用Adam优化器,初始学习率为1×10-4,权重衰减为1×10-5.每个GPU的批大小(batch size)设为4,迭代轮次(epoch)最大值设为100.此外,数据增强包括添加随机噪声、随机翻转和随机旋转.
2.4 评价指标
3 实验结果与分析
为了证明方法对PLNM预测的有效性,进行4组实验.实验中均使用相同的数据预处理和统一的训练策略重新训练所有模型,并调整训练参数以获得最佳性能.
3.1 消融实验
3.1.1 不同组件的有效性
表1 所提方法不同组件的消融分析
Tab.1
| 方法 | (平均值±方差)/% | |||||
|---|---|---|---|---|---|---|
| AUPRC | AUROC | SEN | SPE | ACC | F1 | |
| 基线 | 78.91±6.07 | 90.11±3.21 | 67.02±10.42 | 91.27±2.66 | 84.37±3.99 | 70.73±7.94 |
| 基线+MBALKA | 83.26±4.13 | 91.13±1.79 | 78.07±4.85 | 86.46±6.01 | 84.06±4.48 | 73.15±5.94 |
| 基线+MSFIFA | 81.16±5.21 | 90.82±1.70 | 74.74±15.09 | 87.74±6.22 | 84.04±2.83 | 72.96±6.47 |
| 基线+MBALKA+MSFIFA | 85.44±2.04 | 91.86±2.18 | 73.74±12.20 | 94.33±3.29 | 88.45±2.30 | 78.10±5.38 |
3.1.2 多任务的有效性
为了验证多任务网络的有效性和优越性,进行单任务的PLNM预测实验,并比较了多任务网络中的不确定性权重和等权重损失策略,如表2所示.结果表明,不确定权重有助于平衡分割和分类任务,避免了分割任务在所提方法的训练中占主导地位,从而进一步提高PLNM预测性能.总的来说,所提方法与单独分类任务相比,在AUPRC、AUROC、SEN、SPE、ACC和F1等指标中分别获得了7.31个、2.32个、17.66个、2.22个、6.59个、14.50个百分点的提升,这可能主要是由于原发肿瘤的位置信息和内部异质性特征与PLNM密切相关,从而增强了PLNM预测性能.
表2 所提方法单任务和多任务的消融分析
Tab.2
| 方法 | (平均值±方差)/% | |||||
|---|---|---|---|---|---|---|
| AUPRC | AUROC | SEN | SPE | ACC | F1 | |
| 单任务 | 78.13±5.20 | 89.54±2.50 | 56.08±8.44 | 92.11±4.65 | 81.86±2.98 | 63.60±5.77 |
| 多任务 (等权重) | 82.82±4.54 | 90.69±2.54 | 69.30±16.73 | 90.80±5.72 | 84.68±3.06 | 71.25±7.84 |
| 多任务(不确定权重) | 85.44±2.04 | 91.86±2.18 | 73.74±12.20 | 94.33±3.29 | 88.45±2.30 | 78.10±5.38 |
将多任务网络得到的梯度加权类激活图(Grad-CAM)可视化,如图5所示.其中,图5(a)~5(c)为 mpMRI 影像;黄色箭头表示肿瘤区域;图5(d)和5(e)为Grad-CAMs, 分别通过单任务网络和本文多任务网络获得.图5显示了多任务网络对肿瘤的关注程度,可知单任务网络关注的区域会出现位置偏差,并且关注的范围较为分散;而多任务网络对肿瘤区域关注更准确,对肿瘤内部异质性信息挖掘更充分,因此可以获得更好的PLNM预测结果.
图5

图5
mpMRI影像的二维可视化和相应的Grad-CAMs
Fig.5
Visualization of 2D mpMRI images and corresponding Grad-CAMs
3.2 对比其他经典的单任务分类网络
将多任务网络与其他经典单任务分类网络进行比较,结果如表3所示.所提方法在PLNM预测任务中获得了相当显著的分类性能,优于其他经典单任务分类方法的性能.与单任务方法SeResNet50、CBAMResNet50、DenseNet121、EfficientNet和InceptionV4等相比,所提方法的平均AUPRC提升3.96个百分点,平均AUROC提升2.17个百分点,平均SEN提升5.40个百分点,平均SPE提升5.86个百分点,平均ACC提升5.69个百分点,平均F1提升8.71个百分点.这些单任务方法直接从输入图像中学习与分类任务有关的特征,不可避免地会捕捉到不可靠的特征,从而降低PLNM预测精度.
表3 所提方法与其他经典单任务分类方法对比
Tab.3
| 方法 | (平均值±方差)/% | |||||
|---|---|---|---|---|---|---|
| AUPRC | AUROC | SEN | SPE | ACC | F1 | |
| CBAMResNet50[23] | 78.83±5.01 | 89.33±3.68 | 58.25±12.11 | 90.79±5.12 | 81.55±4.44 | 63.88±9.64 |
| DenseNet121[24] | 82.03±3.38 | 90.24±1.70 | 67.08±11.58 | 90.35±6.25 | 83.73±2.76 | 69.87±5.14 |
| EfficientNet[25] | 80.10±6.68 | 88.25±3.84 | 64.74±5.55 | 87.36±11.00 | 80.93±8.67 | 66.82±10.87 |
| InceptionV4[26] | 83.15±2.13 | 90.31±1.21 | 78.01±9.64 | 81.71±10.11 | 80.67±6.28 | 70.02±6.34 |
| SeResNet50[27] | 83.30±4.80 | 90.30±3.18 | 73.63±2.41 | 92.14±4.50 | 86.88±3.58 | 76.34±5.13 |
| 本文方法 | 85.44±2.04 | 91.86±2.18 | 73.74±12.20 | 94.33±3.29 | 88.45±2.30 | 78.10±5.38 |
3.3 对比其他多任务方法
为了进一步验证所提方法的有效性,将其与其他先进的多任务网络进行比较,结果如表4所示.本文方法在大部分指标上均优于其他3种多任务方法,尤其在AUPRC、SPE、ACC和F1等指标上,提升效果明显, 这表明所提方法实现了更好的PLNM预测性能.
表4 所提方法与其他3种多任务方法对比
Tab.4
| 方法 | (平均值±方差)/% | |||||
|---|---|---|---|---|---|---|
| AUPRC | AUROC | SEN | SPE | ACC | F1 | |
| CMSVNet[12] | 82.68±4.53 | 89.81±2.42 | 81.29±8.49 | 80.32±6.49 | 80.62±2.44 | 70.49±1.49 |
| MTTU-Net[13] | 81.80±6.53 | 91.65±2.41 | 84.62±11.37 | 85.07±11.00 | 84.96±5.79 | 76.58±5.30 |
| PKAF-Net[14] | 78.68±5.16 | 88.52±2.03 | 69.12±11.76 | 91.29±5.08 | 85.00±2.10 | 72.09±4.67 |
| 多任务 (不确定权重) | 85.44±2.04 | 91.86±2.18 | 73.74±12.20 | 94.33±3.29 | 88.45±2.30 | 78.10±5.38 |
4 结语
针对前列腺肿瘤内部异质性信息提取不充分导致的PLNM预测精度较低等问题,提出一种注意力引导多任务学习网络用于PLNM预测.该网络通过共享特征学习,利用任务之间的关联性,能够准确关注肿瘤区域,从而挖掘肿瘤内部异质性特征,此外,通过MBALKA模块提取高层次的语义信息和低层次丰富的细节信息.在PLNM预测网络中通过将共享特征中大尺度特征的丰富细节信息转移到小尺度特征中,获取相应的鉴别性特征.MSFIFA模块则可以有选择地利用多尺度特征来细化单尺度特征.通过捕捉目标的上下文信息,MSFIFA模块能够有效融合不同尺度的特征,从而提高 PLNM 预测的精度.
尽管本文提出的方法在PLNM预测任务中取得了较好的性能,但当前研究的数据来自单一中心,且PLNM阳性患者数量较少,这种数据不平衡的状况可能会进一步限制模型的性能.因此,在未来的工作中,将收集更多PLNM阳性患者数据,以及来自多中心和不同扫描设备的数据,以提高模型的通用性.
参考文献
Cancer statistics, 2022
[J].
Marked prognostic impact of minimal lymphatic tumor spread in prostate cancer
[J].
DOI:S0302-2838(18)30423-8
PMID:29908878
[本文引用: 1]

Nodal metastasis (N1) is a strong prognostic parameter in prostate cancer; however, lymph node evaluation is always incomplete.To study the prognostic value of lymphatic invasion (L1) and whether it might complement or even replace lymph node analysis in clinical practice.Retrospective analysis of pathological and clinical data from 14 528 consecutive patients.Radical prostatectomy.The impact of L1 and N1 on patient prognosis was measured with time to biochemical recurrence as the primary endpoint.Nodal metastases were found in 1602 (12%) of 13 070 patients with lymph node dissection. L1 was seen in 2027 of 14 528 patients (14%) for whom lymphatic vessels had been visualized by immunohistochemistry. N1 and L1 continuously increased with unfavorable Gleason grade, advanced pT stage, and preoperative prostate-specific antigen (PSA) values (p<0.0001 each). N1 was found in 4.3% of 12 501 L0 and in 41% of 2027 L1 carcinomas (p<0.0001). L1 was seen in 11% of 9868 N0 and in 61% of 1360 N1 carcinomas (p<0.0001). Both N1 and L1 were linked to PSA recurrence (p<0.0001 each). This was also true for 17 patients with isolated tumor cells (ie, <200 unequivocal cancer cells without invasive growth) and 193 metastases ≤1mm. Combined analysis of N and L status showed that L1 had no prognostic effect in N1 patients but L1 was strikingly linked to PSA recurrence in N0 patients. N0L1 patients showed a similar outcome as N1 patients.Analysis of lymphatic invasion provides comparable prognostic information than lymph node analysis. Even minimal involvement of the lymphatic system has pivotal prognostic impact in prostate cancer. Thus, a thorough search for lymphatic involvement helps to identify more patients with an increased risk for disease recurrence.Already minimal amounts of tumor cells inside the lymph nodes or intraprostatic lymphatic vessels have a severe impact on patient prognosis.Copyright © 2018 European Association of Urology. Published by Elsevier B.V. All rights reserved.
前列腺癌淋巴结转移分子机制的研究进展
[J].
Progress of molecular mechanism leading to lymph node metastasis in prostate cancer
[J].
Predictive value of MRI in the localization, staging, volume estimation, assessment of aggressiveness, and guidance of radiotherapy and biopsies in prostate cancer
[J].
3.0 T MR扩散加权成像ADC值及ROC曲线分析对前列腺癌淋巴结转移的诊断价值
[J].
Value of 3.0 T MR diffusion-weighted imaging and ROC curve in diagnosis of lymph node metastasis in patients with prostate cancer
[J].
Preoperative multiparametric MRI of the prostate for the prediction of lymph node metastases in prostate cancer patients treated with extended pelvic lymph node dissection
[J].
DOI:10.1007/s00330-017-5229-6
PMID:29270644
[本文引用: 1]
To assess the role of preoperative multiparametric MRI (mpMRI) of the prostate in the prediction of nodal metastases in patients treated with radical prostatectomy (RP) and extended pelvic lymph node dissection (ePLND).We retrospectively analyzed 101 patients who underwent both preoperative mpMRI of the prostate and RP with ePLND at our institution. For each patient, complete preoperative clinical data and tumour characteristics at mpMRI were recorded. Final histopathologic stage was considered the standard of reference. Univariate and multivariate logistic regression analyses were performed.Nodal metastases were found in 23/101 (22.8%) patients. At univariate analyses, all clinical and radiological parameters were significantly associated to nodal invasion (all p<0.03); tumour volume at MRI (mrV), tumour ADC and tumour T-stage at MRI (mrT) were the most accurate predictors (AUC = 0.93, 0.86 and 0.84, respectively). A multivariate model including PSA levels, primary Gleason grade, mrT and mrV showed high predictive accuracy (AUC = 0.956). Observed prevalence of nodal metastases was very low among tumours with mrT2 stage and mrV<1cc (1.8%).Preoperative mpMRI of the prostate can predict nodal metastases in prostate cancer patients, potentially allowing a better selection of candidates to ePLND.• Multiparametric-MRI of the prostate can predict nodal metastases in prostate cancer • Tumour volume and stage at MRI are the most accurate predictors • Prevalence of nodal metastases is low for T2-stage and <1cc tumours • Preoperative mpMRI may allow a better selection of candidates to lymphadenectomy.
Indication to pelvic lymph nodes dissection for prostate cancer: The role of multiparametric magnetic resonance imaging when the risk of lymph nodes invasion according to Briganti updated nomogram is 5
[J].
Eliminating microscopic lymph node metastasis by performing pelvic lymph node dissection during radical prostatectomy for prostate cancer
[J].
DOI:10.3892/mco.2019.1965
PMID:31929879
[本文引用: 1]
The oncological benefit of pelvic lymph node dissection (PLND) for prostate cancer (PCa) remains unclear. The therapeutic effect of PLND on the elimination of microscopic metastases during radical prostatectomy (RP) for PCa was examined in the current study. A total of 348 Japanese patients with high- or intermediate-risk PCa without lymph node metastasis, who underwent antegrade RP at the Kyushu Cancer Center (Fukuoka, Japan) between August 1998 and May 2013 were retrospectively analyzed. The patients were divided into the standard (obturator + internal iliac nodes) group and the expanded (standard + additional nodes) group according to the extent of PLND. Preoperative and postoperative characteristics were also analyzed to determine the factors associated with prostate-specific antigen (PSA) failure. Standard and expanded PLND were performed in 70.9% (247/348) and 29.1% (101/348) of cases, respectively. The results revealed that preoperative PSA levels were the only marked difference between the two groups. No differences were observed in the other preoperative and postoperative characteristics. Furthermore, the rate of PSA recurrence in each group did not differ to a statistically significant extent (P=0.3622). Reducing the area of dissection from expanded PLND to standard PLND significantly reduced the number of dissected lymph nodes (P<0.0001). Additionally, the PSA level, clinical tumor stage, Gleason score of the biopsy specimen, pathological tumor stage and extent of PLND were all associated with PSA recurrence, as determined via multivariate Cox hazards regression analysis (P=0.0177, P=0.0023, P=0.0027, P<0.0001 and P=0.0164, respectively). In high- and intermediate-risk patients without lymph node metastasis, a greater number of lymph nodes were dissected when the extent of dissection was greater. Furthermore, the extent of PLND was a significantly associated with PSA failure. The results indicated that PLND exerted a therapeutic effect by eliminating microscopic pelvic lymph node metastases that were not detected by routine pathological examinations.Copyright: © Furubayashi et al.
Utility of diffusion weighted imaging-based radiomics nomogram to predict pelvic lymph nodes metastasis in prostate cancer
[J].
DOI:10.1186/s12880-022-00905-3
PMID:36333664
[本文引用: 1]
Preoperative pelvic lymph node metastasis (PLNM) prediction can help clinicians determine whether to perform pelvic lymph node dissection (PLND). The purpose of this research is to explore the feasibility of diffusion-weighted imaging (DWI)-based radiomics for preoperative PLNM prediction in PCa patients at the nodal level.The preoperative MR images of 1116 pathologically confirmed lymph nodes (LNs) from 84 PCa patients were enrolled. The subjects were divided into a primary cohort (67 patients with 192 positive and 716 negative LNs) and a held-out cohort (17 patients with 43 positive and 165 negative LNs) at a 4:1 ratio. Two preoperative pelvic lymph node metastasis (PLNM) prediction models were constructed based on automatic LN segmentation with quantitative radiological LN features alone (Model 1) and combining radiological and radiomics features (Model 2) via multiple logistic regression. The visual assessments of junior (Model 3) and senior (Model 4) radiologists were compared.No significant difference was found between the area under the curve (AUCs) of Models 1 and 2 (0.89 vs. 0.90; P = 0.573) in the held-out cohort. Model 2 showed the highest AUC (0.83, 95% CI 0.76, 0.89) for PLNM prediction in the LN subgroup with a short diameter ≤ 10 mm compared with Model 1 (0.78, 95% CI 0.70, 0.84), Model 3 (0.66, 95% CI 0.52, 0.77), and Model 4 (0.74, 95% CI 0.66, 0.88). The nomograms of Models 1 and 2 yielded C-index values of 0.804 and 0.910, respectively, in the held-out cohort. The C-index of the nomogram analysis (0.91) and decision curve analysis (DCA) curves confirmed the clinical usefulness and benefit of Model 2.A DWI-based radiomics nomogram incorporating the LN radiomics signature with quantitative radiological features is promising for PLNM prediction in PCa patients, particularly for normal-sized LNM.© 2022. The Author(s).
Multiparametric MRI-based radiomics model to predict pelvic lymph node invasion for patients with prostate cancer
[J].
DOI:10.1007/s00330-022-08625-6
PMID:35238971
[本文引用: 1]
To identify which patient with prostate cancer (PCa) could safely avoid extended pelvic lymph node dissection (ePLND) by predicting lymph node invasion (LNI), via a radiomics-based machine learning approach.An integrative radiomics model (IRM) was proposed to predict LNI, confirmed by the histopathologic examination, integrating radiomics features, extracted from prostatic index lesion regions on MRI images, and clinical features via SVM. The study cohort comprised 244 PCa patients with MRI and followed by radical prostatectomy (RP) and ePLND within 6 months between 2010 and 2019. The proposed IRM was trained in training/validation set and evaluated in an internal independent testing set. The model's performance was measured by area under the curve (AUC), sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV). AUCs were compared via Delong test with 95% confidence interval (CI), and the rest measurements were compared via chi-squared test or Fisher's exact test.Overall, 17 (10.6%) and 14 (16.7%) patients with LNI were included in training/validation set and testing set, respectively. Shape and first-order radiomics features showed usefulness in building the IRM. The proposed IRM achieved an AUC of 0.915 (95% CI: 0.846-0.984) in the testing set, superior to pre-existing nomograms whose AUCs were from 0.698 to 0.724 (p < 0.05).The proposed IRM could be potentially feasible to predict the risk of having LNI for patients with PCa. With the improved predictability, it could be utilized to assess which patients with PCa could safely avoid ePLND, thus reduce the number of unnecessary ePLND.• The combination of MRI-based radiomics features with clinical information improved the prediction of lymph node invasion, compared with the model using only radiomics features or clinical features. • With improved prediction performance on predicting lymph node invasion, the number of extended pelvic lymph node dissection (ePLND) could be reduced by the proposed integrative radiomics model (IRM), compared with the existing nomograms.© 2022. The Author(s), under exclusive licence to European Society of Radiology.
Integration of clinicopathologic identification and deep transferrable image feature representation improves predictions of lymph node metastasis in prostate cancer
[J].
Multi-task learning for segmentation and classification of tumors in 3D automated breast ultrasound images
[J].
A fully automated multimodal MRI-based multi-task learning for glioma segmentation and IDH genotyping
[J].
Prior knowledge-aware fusion network for prediction of macrovascular invasion in hepatocellular carcinoma
[J].
Optimized U-net for brain tumor segmentation
[C]//
Visual attention network
[J].
Attention is all you need
[C]//
Multi-task learning using uncertainty to weigh losses for scene geometry and semantics
[C]//
Elastix: A toolbox for intensity-based medical image registration
[J].
DOI:10.1109/TMI.2009.2035616
PMID:19923044
[本文引用: 1]
Medical image registration is an important task in medical image processing. It refers to the process of aligning data sets, possibly from different modalities (e.g., magnetic resonance and computed tomography), different time points (e.g., follow-up scans), and/or different subjects (in case of population studies). A large number of methods for image registration are described in the literature. Unfortunately, there is not one method that works for all applications. We have therefore developed elastix, a publicly available computer program for intensity-based medical image registration. The software consists of a collection of algorithms that are commonly used to solve medical image registration problems. The modular design of elastix allows the user to quickly configure, test, and compare different registration methods for a specific application. The command-line interface enables automated processing of large numbers of data sets, by means of scripting. The usage of elastix for comparing different registration methods is illustrated with three example experiments, in which individual components of the registration method are varied.
nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation
[J].
DOI:10.1038/s41592-020-01008-z
PMID:33288961
[本文引用: 1]
Biomedical imaging is a driver of scientific discovery and a core component of medical care and is being stimulated by the field of deep learning. While semantic segmentation algorithms enable image analysis and quantification in many applications, the design of respective specialized solutions is non-trivial and highly dependent on dataset properties and hardware conditions. We developed nnU-Net, a deep learning-based segmentation method that automatically configures itself, including preprocessing, network architecture, training and post-processing for any new task. The key design choices in this process are modeled as a set of fixed parameters, interdependent rules and empirical decisions. Without manual intervention, nnU-Net surpasses most existing approaches, including highly specialized solutions on 23 public datasets used in international biomedical segmentation competitions. We make nnU-Net publicly available as an out-of-the-box tool, rendering state-of-the-art segmentation accessible to a broad audience by requiring neither expert knowledge nor computing resources beyond standard network training.
The precision-recall plot is more informative than the ROC plot when evaluating binary classifiers on imbalanced datasets
[J].
The impact of class imbalance in classification performance metrics based on the binary confusion matrix
[J].
An improved ResNet algorithm based on CBAM
[C]//
Densely connected convolutional networks
[C]//
EfficientNet: Rethinking model scaling for convolutional neural networks
[C]//
Inception-v4, inception-ResNet and the impact of residual connections on learning
[C]//
Squeeze-and-excitation networks
[C]//

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}